The U.S. Preventive Services Task Force (USPSTF) has released a new advisory statement outlining the group’s position regarding the use of statin therapy for the primary prevention of cardiovascular disease in adult patients.
Released Aug. 23, the 8-page recommendation statement, which serves as an update to the group’s 2016 recommendation statement on the topic, recommends the use of statins for the primary prevention of cardiovascular disease among adults ages 40 to 75. years who have 1 or more cardiovascular disease risk factors and an estimated 10-year CVD risk of 10% or more, while selective offering of statin therapy for primary prevention is recommended among adults aged 40 to 75 years with 1 or more risk factors and an estimated 10-year risk of 7.5% to less than 10%.
“In summary, the new USPSTF recommendations for statin therapy are consistent with current AHA/ACC/MS guidelines that patients aged 40 to 75 years with a sufficiently high risk of 10-year ASCVD deserve statin therapy.” statins,” the trio wrote. “There is disagreement about the recommended thresholds for statin initiation and how the physician and patient resolve the common situation in which an estimate of risk makes treatment decisions uncertain.”
In this review, the results suggested that statins were significantly associated with a lower risk of all-cause mortality (RR, 0.92 [95% CI, 0.87 to 0.98]; ARD, -0. 35% [95% CI, -0.57 to -0.14%]), stroke (RR, 0.78 [95% CI, 0.68 to 0.90]; ARD, −0.39 % [95% CI, −0.54 to −0.25%]), myocardial infarction (RR, 0.67 [95% CI, 0.60 to 0.75] ARD, -0.85% [95% CI, 95%, -1.22% to -0.47%]) and composite cardiovascular outcomes (RR, 0.72 [95% CI, 0.64 to 0.81]; ARD, -1.28% [95% %, -1.61 to −0.95%]), but the association with cardiovascular mortality was not statistically significant (RR, 0.91 [95% CI, 0.81 to 1.02]; ARD, −0 .13%).
When evaluating the benefits versus harms of statin therapy, the results indicated that statin therapy was not significantly associated with an increased risk of serious adverse events (RR, 0.97 [95% CI, 0.93 to 1 .01]), myalgia (RR, 0.98 [95% CI, 0.86 to 1.11]),
The researchers noted that a single trial found that high-intensity statin therapy was significantly associated with increased risk, but there were no clear differences in outcomes based on statin therapy outside of this case. Later in their evidence report, the authors noted that the benefits seen in the review were consistent across patient subgroups, but data for patients over 75 years of age were sparse.
Importance
A 2016 review for the US Preventive Services Task Force (USPSTF) found that statin use for primary prevention of cardiovascular disease (CVD) was associated with reduced mortality and cardiovascular outcomes.
Aim
Update 2016 review on statins for primary prevention of CVD to report to USPSTF
Data sources
Ovid MEDLINE, Cochrane Central Register of Controlled Trials and Cochrane Database of Systematic Reviews (until November 2021); surveillance until May 20, 2022.
Study selection
Randomized clinical trials of statins versus placebo or no statin and statin intensity in adults without prior cardiovascular events; large cohort studies on harms.
Data extraction and synthesis
One researcher extracted the data; a second checked the accuracy. Two investigators independently rated study quality.
Main results and measures
Cardiovascular and all-cause mortality, myocardial infarction, stroke, composite cardiovascular outcomes, and adverse events.
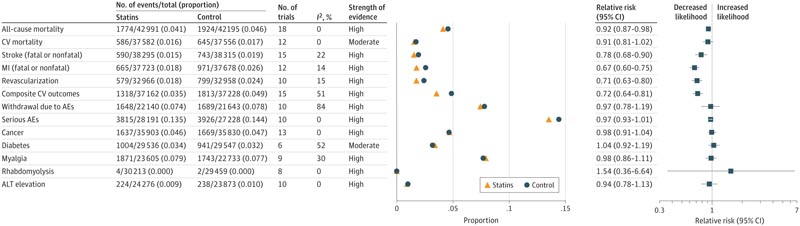
AE indicates adverse event; ALT, alanine aminotransferase; CV, cardiovascular; MA, meta-analysis; MI, myocardial infarction; RR, relative risk; SOE, strength of evidence.
Conclusions and relevance
In adults at increased risk for CVD but without prior CVD events, statin therapy for primary prevention of CVD was associated with a reduced risk of all-cause mortality and CVD events. The benefits of statin therapy appear to be present in diverse clinical and demographic populations, with relative benefits consistent in groups defined by clinical and demographic characteristics.















