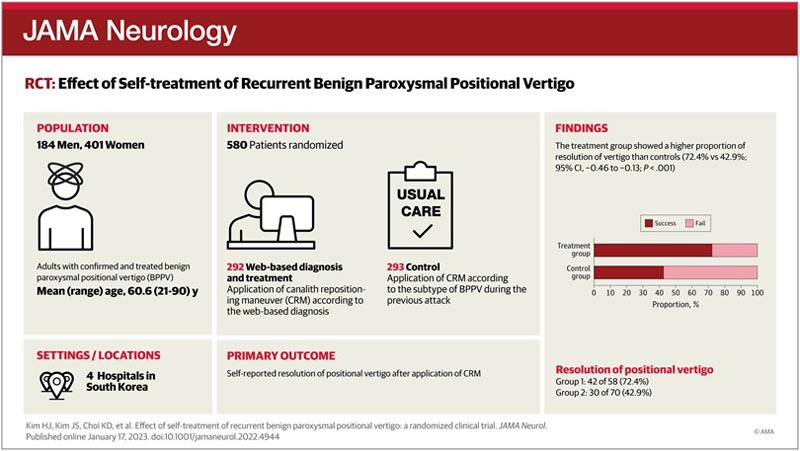
Key points Ask Is web-guided diagnosis and treatment in recurrent benign paroxysmal positional vertigo (BPPV) feasible and effective? Findings In this randomized clinical trial of 585 patients, patients in the treatment group, who performed the canalith repositioning maneuver according to the web-based diagnosis of the subtype of recurrent benign paroxysmal positional vertigo (BPPV), showed a higher proportion of vertigo resolution than the controls, who applied the canalicular repositioning maneuver according to the BPPV subtype during the previous attack (72.4% vs 42.9%). Meaning Patients can benefit from self-performed benign recurrent paroxysmal positional vertigo (BPPV) treatment using a web-guided system. |
Importance
Benign paroxysmal positional vertigo (BPPV) is the most common cause of vertigo with frequent recurrences.
Aim
To determine the effectiveness of a web-based diagnosis and treatment of BPPV when it recurs in patients with confirmed and treated BPPV.
Design, scope and participants
This randomized, controlled, parallel-group, double-blind trial was conducted at multiple referral university hospitals in South Korea between July 2017 and February 2020.
Of 728 patients (age ≥20 years) diagnosed with and treated with BPPV, 585 were enrolled after excluding 143 who refused to participate, could not use the Internet, or had spinal problems, multichannel BPPV, or cognitive dysfunction. Patients were followed for recurrence for at least 2 years until February 2022.
Interventions
Patients were randomly assigned (1:1) to the treatment or control group. Patients in the treatment group completed a diagnostic questionnaire and received a video clip for self-administration of the canalicular repositioning maneuver (CRM) according to the type of BPPV diagnosed when they experienced positional vertigo again.
Patients in the control group received a video clip for CRM self-administration according to the type of BPPV that had been diagnosed at the time of enrollment.
Editor’s note Canalicular repositioning maneuver General description The canalicular repositioning procedure can treat benign paroxysmal positional vertigo. Benign paroxysmal positional vertigo is a condition that causes brief but intense sensations of dizziness and spinning. These sensations are also known as vertigo. They can occur when you move your head. Vertigo is usually the result of a problem in the part of the inner ear responsible for balance. Benign paroxysmal positional vertigo occurs when small particles called canaliths or otoconia that are in a part of the inner ear become loose and fall out. They often move in the semicircular canals of the inner ear. This can cause sensitivity to motion and vertigo. The canalicular repositioning procedure can move these particles to a part of the ear where they will not cause dizziness. The procedure consists of a series of simple head movements. It can be done in the healthcare provider’s office. The procedure is usually effective. The procedure relieves vertigo in about 80% of people after one or two treatments. However, the problem can happen again. |

For self-treatment of recurrent benign paroxysmal positional vertigo (BPPV), a web-based questionnaire was provided to access using a computer or smartphone whenever patients developed vertigo. After completing the questionnaire, a video clip was provided for patients to perform the canalith repositioning maneuver (CRM) by themselves. These video clips included audio instructions for the proper functioning of the CRM in real time. This is one of several videos provided on the web, CRM for Right Posterior Canal BPPV. Click here to access the demonstration video .
Main results and measures
The primary outcome was self-reported resolution of positional vertigo following CRM. Secondary outcomes included difficulties and need for assistance when using the program and any falls or other CRM-related adverse events. The primary outcome was analyzed using intention-to-treat and per-protocol methods.
Results
Of 585 patients enrolled, 292 were randomized to the treatment group (mean [SD] age, 60.3 [12.8] years, 37 [64%] female) and 293 were randomized to the control group (mean [SD] age , 61.1 [13.2] years; 50 [71%] women).
Overall, 128 (21.9%) had recurrence (58 in the treatment group and 70 in the control group) and 109 (85.2%) successfully used the web-based system.
In the intention-to-treat analysis, 42 of 58 individuals (72.4%) in the treatment group and 30 of 70 individuals (42.9%) in the control group reported resolution of vertigo (χ 2 test: CI 95%, 0.13-0.46; p < 0.001).
Conclusions and relevance
This trial demonstrated the effectiveness of a web-based system for the diagnosis and treatment of recurrent BPPV. The use of this system can play an important role in telemedicine for vestibular disorders.
Trial registration: Clinical Research Information Service Identifier: KCT0002364















