We use cookies to ensure you have the best browsing experience on our website. By using our site, you acknowledge that you have read and understood our Cookie Policy & Privacy Policy
Antithrombotic Therapy for Ischemic Stroke Prevention
Evaluating the balance between the benefits of antithrombotic therapies for preventing ischemic stroke and their associated increased risk of bleeding.
Stroke is a devastating condition with significant morbidity and mortality worldwide. Antithrombotic therapy plays a crucial role in the primary and secondary prevention of stroke.
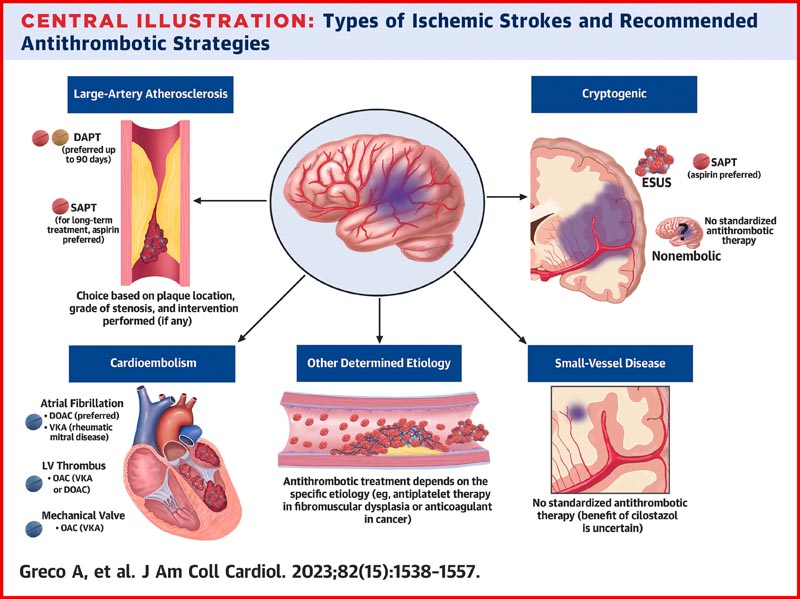
Single or dual antiplatelet therapy is generally preferred in cases of large artery atherosclerosis and small vessel disease, while anticoagulation is recommended in conditions of blood stasis or hypercoagulable states that mostly result in red thrombi. However, the benefit of antithrombotic therapies must be weighed against the increased risk of bleeding, which can pose significant challenges in the pharmacological treatment of this condition.
The following are key points to remember from a review of the latest advances on antithrombotic therapy for the primary and secondary prevention of ischemic stroke:
Decisions regarding antithrombotic treatment in primary and secondary stroke prevention should always involve consideration of the bleeding risk of each individual patient.
The default treatment for secondary stroke prevention should be an antiplatelet agent monotherapy, usually initiated within 24 to 48 hours of symptom onset.
Dual antiplatelet therapy (DAPT) is indicated for a short period (~21 days) after a minor acute ischemic stroke or transient ischemic attack. Antiplatelet monotherapy should be initiated after completion of the short course of DAPT.
Ischemic stroke patients with nonvalvular atrial fibrillation (AF) and no contraindications should receive anticoagulation with a DOAC or warfarin.
Decisions regarding the timing of initiation or reinitiation of anticoagulation for AF after ischemic stroke should be based on infarct size, evidence of hemorrhagic transformation, and patient-specific factors (e.g., presence of venous thrombosis). profound comorbid).
The treatment of choice for secondary prevention of stroke after ESUS ( embolic stroke of undetermined origin ) is antiplatelet monotherapy.
Anticoagulation is generally the antithrombotic treatment of choice for antiphospholipid antibody syndrome and for recurrent ischemic stroke suspected to be secondary to hypercoagulability related to malignancy.
In the first 3 months after a vertebral or carotid artery dissection, aspirin or warfarin may be used.
Anticoagulation with warfarin is the treatment of choice for left ventricular thrombus to prevent stroke and/or systemic embolism.