
 COVID-19 leads to a several times higher risk of blood clots and cerebral venous thrombosis (CVT) than current COVID-19 vaccines.
COVID-19 leads to a several times higher risk of blood clots and cerebral venous thrombosis (CVT) than current COVID-19 vaccines.
Researchers at the University of Oxford reported today that the risk of rare blood clotting known as cerebral venous thrombosis (CVT) after COVID-19 infection is around 100 times higher than normal, several times higher than after vaccination or after the flu. .
The study authors, led by Professor Paul Harrison and Dr Maxime Taquet from the Department of Psychiatry at the University of Oxford and the Oxford NIHR Health Biomedical Research Centre, counted the number of CVT cases diagnosed in the two weeks after the diagnosis of COVID-19, or after the dose of a vaccine. They then compared these to the estimated incidences of CVT after influenza and the baseline level in the general population.
- They report that CVT is more common after COVID-19 than in any of the comparison groups, and 30% of these cases occur in those under 30 years of age.
- Compared to current COVID-19 vaccines, this risk is 8 to 10 times higher , and compared to the population baseline, approximately 100 times higher.
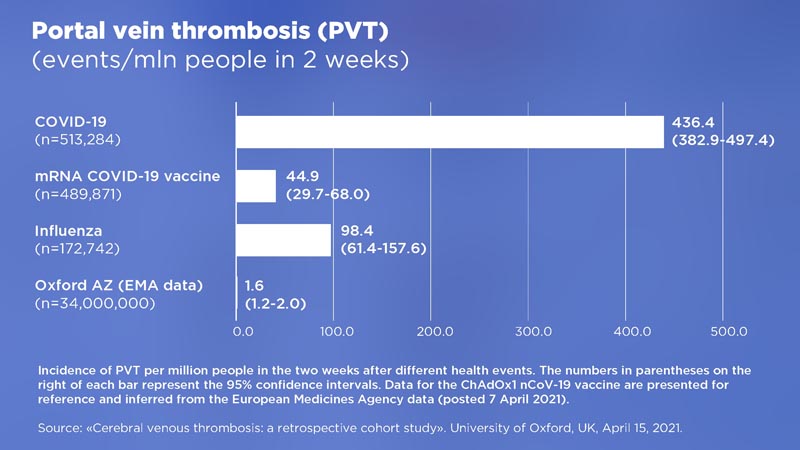
The breakdown comparison of reported cases of CVT in patients with COVID-19 compared to cases of CVT in those who received a COVID-19 vaccine is:
|
However, all comparisons should be interpreted with caution as the data is still increasing.
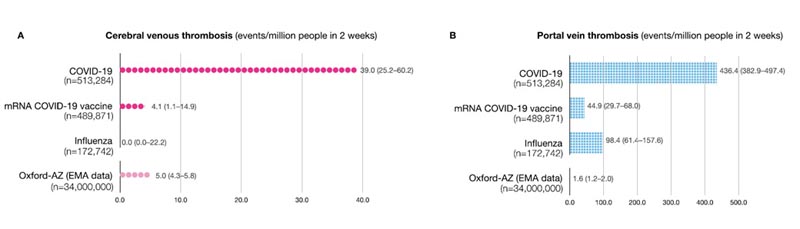
Incidence of CVT (A) and DVT (B) per million people in the two weeks after different health events. The numbers in parentheses to the right of each bar represent the 95% confidence intervals. ChAdOx1 nCoV-19 vaccine data are presented for reference and inferred from European Medicines Agency data (published April 7, 2021).
Paul Harrison, professor of psychiatry and director of the Translational Neurobiology Group at the University of Oxford, said: “There are concerns about possible associations between vaccines and CVT, leading governments and regulators to restrict the use of certain vaccines. . However, one key question remained unknown: “What is the risk of CVT after a COVID-19 diagnosis?”
“We have reached two important conclusions.
- First, COVID-19 markedly increases the risk of CVT, adding to the list of blood clotting problems caused by this infection.
- Second, the risk of COVID-19 is higher than we see with current vaccines, even for those under 30; something that should be taken into account when considering the balances between risks and benefits of vaccination.”
Dr Maxime Taquet, also from the Translational Neurobiology Group, said: ’It is important to note that these data should be interpreted with caution, especially as the data on the Oxford-AstraZeneca vaccine comes from EMA monitoring, while the other data They use records from the TriNetX electronic health network. However, the signs that COVID-19 is related to CVT, as well as portal vein thrombosis, a liver clotting disorder, are clear and we should take note of them.’
An important factor that requires further investigation is whether COVID-19 and vaccines cause CVT by the same mechanism or by different mechanisms. There may also be underreporting or miscoding of CVT in medical records and therefore uncertainty as to the accuracy of the results.















