
Prevention of cardiovascular disease remains an important public health issue, with well-documented associations between cardiovascular risk factors in adulthood and cardiovascular events.
Despite interest in childhood risk factors and subsequent cardiovascular disease in adults, as recently reviewed, findings from longitudinal studies beginning with the assessment of childhood risk factors have generally been restricted to associations with subclinical disease in adulthood.
The possibility of expanding the findings to include associations with cardiovascular events in adults has been hampered by the lack of cohorts with complete childhood data available on anthropometric measurements, blood pressure and laboratory values, and with follow-up carried out until ages at which the cardiovascular events become predominant.
Childhood cardiovascular risk factors predict subclinical cardiovascular disease in adults, but links to clinical events are unclear.
In a prospective cohort study involving participants from the International Children’s Cardiovascular Cohort Consortium (i3C), we assessed whether childhood risk factors (at ages 3 to 19 years) were associated with cardiovascular events in adulthood after a average follow-up of 35 years.
Body mass index, systolic blood pressure, total cholesterol level, triglyceride level, and youth smoking were analyzed using age- and sex-specific z-scores derived from i3C and with a risk z-score. combined which was calculated as the average unweighted index of the five risk z scores.
An algebraically comparable adult combined risk z score (before any cardiovascular event) was analyzed along with childhood risk factors. The study outcomes were fatal cardiovascular events and fatal or non-fatal cardiovascular events,
In the analysis of 319 fatal cardiovascular events that occurred among 38,589 participants (49.7% men and 15.0% black; mean [±SD] age at childhood visits, 11.8±3.1 years), the ratios Hazard risk ratios for a fatal cardiovascular event in adulthood ranged from 1.30 (95% confidence interval [CI], 1.14 to 1.47) per unit increase in the z score for total cholesterol level to 1.61 (95% CI, 1.21 to 2.13) for young smokers (yes vs. no).
The hazard ratio for a fatal cardiovascular event with respect to the combined risk z score was 2.71 (95% CI, 2.23 to 3.29) per unit increase.
The hazard ratios and their 95% confidence intervals in the analyzes of fatal cardiovascular events were similar to those in the analyzes of 779 fatal or nonfatal cardiovascular events that occurred among 20,656 participants who could be evaluated for this outcome.
In the analysis of 115 fatal cardiovascular events that occurred in a subgroup of 13,401 participants (age 31.0 ± 5.6 years at adult measurement) who had data on adult risk factors, the hazard ratio adjusted for the children’s combined risk z score was 3.54 (95% CI, 2.57 to 4.87) per unit increase, and the mutually adjusted hazard ratio for the change in Combined risk z score from childhood to adulthood was 2.88 (95% CI, 2.06 to 4.05) per unit increase.
The results were similar in the analysis of 524 fatal or non-fatal cardiovascular events. 87) per unit increase, and the mutually adjusted hazard ratio for the change in the pooled risk z score from childhood to adulthood was 2.88 (95% CI, 2.06 to 4. 05) per unit of increase.
The results were similar in the analysis of 524 fatal or non-fatal cardiovascular events. 87) per unit increase, and the mutually adjusted hazard ratio for the change in the pooled risk z score from childhood to adulthood was 2.88 (95% CI, 2.06 to 4. 05) per unit of increase. The results were similar in the analysis of 524 fatal or non-fatal cardiovascular events.
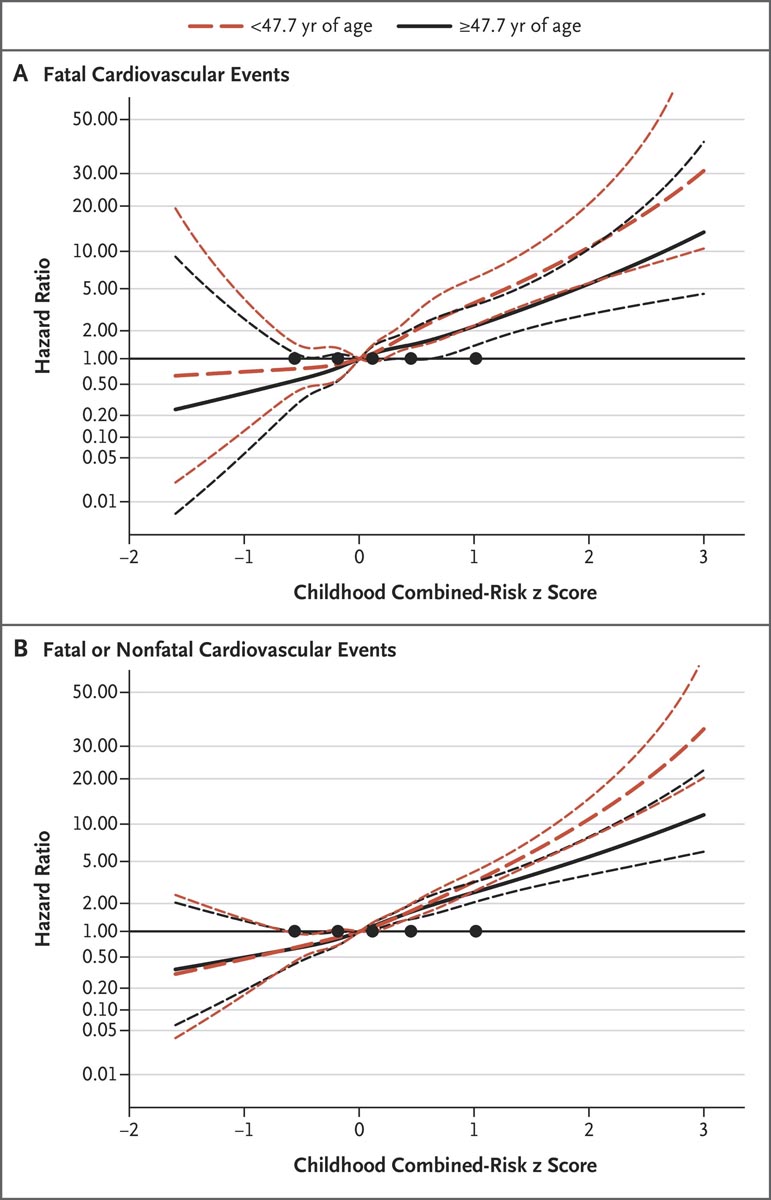
Risk ratios for cardiovascular events at younger and older ages. Panel A shows the hazard ratios for fatal cardiovascular events and Panel B shows the hazard ratios for fatal or nonfatal cardiovascular events. The hazard ratio spline is presented on a logarithmic scale across the distribution of infant combined risk z scores, with 95% confidence intervals (shorter dashed lines). The youngest age (<47.7 years) includes all participants, among whom there were 157 fatal events and a mean of 797 fatal or non-fatal events among imputations. The older group includes only participants who were followed up and had no events or had events at or after 47.7 years of age (a total of 18,352 participants, among whom 162 had a fatal cardiovascular event and 1,049 had a fatal event due to other causes or were not followed beyond the age of 47.6 years; the remaining 17,141 participants had a mean of 766 fatal or non-fatal events at imputation). Black circles indicate nodes located at the 5th, 25th, 50th, 75th, and 95th percentiles of the combined risk z score.
This prospective cohort study showed that the cardiovascular risk factors of body mass index, systolic blood pressure, total cholesterol level, triglyceride level and youth smoking, particularly in combination from early childhood, were associated with events. cardiovascular diseases in adults and death from cardiovascular causes before the age of 60 years.
(Funded by the National Institutes of Health).















