
Multiparametric MRI Evaluation of VI-RADS for Bladder Tumors Located at the Ureteral Orifice Summary The bladder imaging data and reporting system could be used to accurately detect detrusor muscle invasion in patients with bladder cancer occurring at the ureteral orifices. Background The Bladder Imaging Reporting and Data System (VI-RADS), based on multiparametric MRI scans, standardizes preoperative staging of bladder cancer. However, limitations have been reported for VI-RADS, particularly for ureteral orifice tumors. Aim To investigate the diagnostic performance and interobserver agreement of VI-RADS in the evaluation of muscle invasion by bladder tumors located at the ureteral orifice. Materials and methods In this retrospective study , patients with histopathologically confirmed bladder cancer at the ureteral orifice were analyzed from January 2012 to November 2021. Two blinded radiologists independently scored multiparametric MRI scans according to VI-RADS. Interobserver agreement of VI-RADS scores was assessed with weighted κ analysis. Receiver operating characteristic curve analysis was used to evaluate the diagnostic performance of VI-RADS scores in predicting muscle invasion. Results A total of 78 patients (mean age, 67 years ± 7 [SD]; age range, 46–90 years; 67 men) were included in the final analysis: 25 with nonmuscle-invasive bladder cancer and 53 with bladder cancer. with muscle invasive bladder cancer (MIBCa). In the consensus reading, one (1%) case was graded as VI-RADS 1, 27 cases (35%) were graded as VI-RADS 2, six (8%) were graded as VI-RADS 3, 10 (13 %) were rated as VI-RADS 4, and 34 (44%) were rated as VI-RADS 5. Comparing the VI-RADS score with histopathological findings, the presence of muscle invasion was confirmed to be 0% (zero out of one) for VI-RADS 1, 15% (four of 27) for VI-RADS 2, 83%. (five of six) for VI-RADS 3, 100% (10 of 10) for VI-RADS 4, and 100% (34 of 34) for VI-RADS 5. The area under the VI-RADS receiver operating characteristic curve in MIBCa detection was 0.96 (95% CI: 0.92, 1.00). Conclusion The bladder imaging data and reporting system could be used to accurately predict muscle invasion of bladder tumors occurring at the ureteral orifice. |
Comments
Bladder cancer is the most common malignancy of the urinary system and is associated with a high recurrence rate.
Bladder cancers in the ureteral orifice have a higher frequency of invasion of the detrusor muscle
Bladder cancer treatment depends on the status of muscle invasion. Non-muscle-invasive bladder cancer (NMIBCa) is usually low grade, while muscle-invasive bladder cancer (MIBCa) is an aggressive tumor with a poor prognosis and requires more intensive treatment.
Imaging is required to provide accurate preoperative characterization of muscle invasion. Recent developments in MRI have made multiparametric MRI an important adjunct to transurethral resection of bladder tumor.
The Bladder Imaging Reporting and Data System (VI-RADS) provides a five-point MRI score to predict the likelihood of muscle infiltration by bladder cancer. However, the VI-RADS criteria were reported to have limitations, particularly for tumors located at the ureteral orifices.
"Numerous studies have shown that VI-RADS is an effective comprehensive tool in the detection of muscle invasion by bladder cancer," according to Huanjun Wang, MD, PhD, of the Department of Radiology, The First Affiliated Hospital, Sun Yat-Sen University . , in Canton, China. "We wanted to see if VI-RADS could be used to accurately predict muscle invasion of tumors occurring at the ureteral orifice, a specific anatomical location with a higher frequency of tumor invasion of the detrusor muscle."
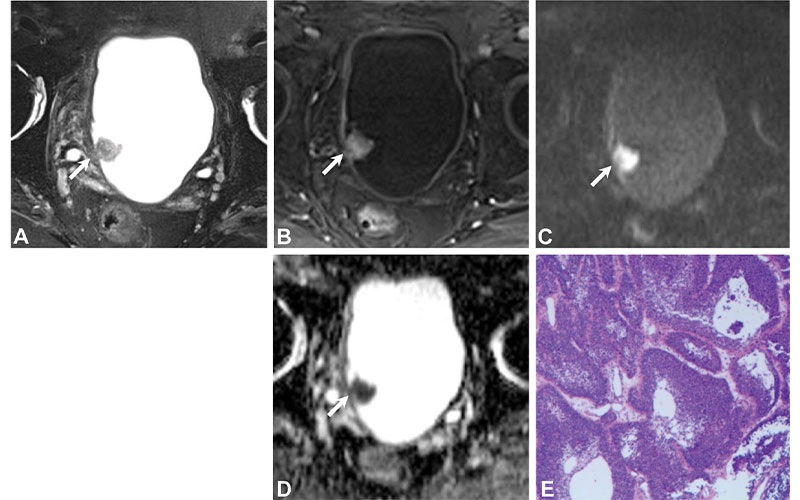
Wang Radiology Bladder Cancer Fig 3 Images in an 86-year-old man with pTa low-grade urothelial carcinoma. (A) Axial T2-weighted image shows a tumor over the right ureteral orifice with a hydroureter. Disruption of low signal intensity muscularis propria is unclear (arrow). (B) Axial contrast-enhanced image shows no early enhancement of the muscularis propria (arrow). Axial (C) diffusion-weighted and (D) apparent diffusion coefficient images show no clear disruption of the low-signal intensity muscularis propria (arrow). The final bladder imaging data and reporting system score was 3 for all readers. (E) The histopathological image obtained after transurethral resection shows that no invasion of the detrusor muscle is found. (Hematoxylin-eosin stain; original magnification, ×100.) https://doi.org/10.1148/radiol.220028 © RSNA 2022
Radiologists were able to match VI-RADS staging
In this retrospective study, patients with histopathologically confirmed bladder cancer occurring at the ureteral orifice were analyzed. Two blinded radiologists independently scored the multiparametric MRI scans according to VI-RADS.
A total of 78 patients were included in the final analysis: 25 with NMIBCa and 53 with MIBCa. In the consensus reading, one case (1%) was graded as VI-RADS 1, 27 cases (35%) were graded as VI-RADS 2, six (8%) were graded as VI-RADS 3, 10 (13 %) were scored as VI-RADS 4, and 34 (44%) were scored as VI-RADS.
Comparing the VI-RADS score with histopathological findings, the presence of muscle invasion was confirmed to be 0% (zero out of one) for VI-RADS 1, 15% (four of 27) for VI-RADS 2, 83%. (five of six) for VI-RADS 3, 100% (10 of 10) for VI-RADS 4, and 100% (34 of 34) for VI-RADS 5. The area under the receiver operating characteristic curve (AUC) of VI-RADS in the detection of MIBCa was 0.96, indicating high accuracy of the diagnostic test.
“Currently, bladder cancer staging is achieved through a combination of examinations, transurethral resection of bladder tumor specimens, and imaging. However, the quality of transurethral resection of bladder tumors often varies among surgeons and may miss muscle infiltration in up to 25% of invasive cancers. Therefore, there is an urgent need to develop an accurate and non-invasive method to assess muscle invasion in bladder cancer,” said co-author Yan Guo, MD, PhD, also of Sun Yat-Sen University. “The area under the receiver operating characteristic curve of VI-RADS in detecting MIBCa was high, suggesting that VI-RADS can accurately distinguish non-muscle-invasive and muscle-invasive bladder cancer before surgery.” and provide a powerful tool for patients. to choose treatment modalities.”
Accurately determining the muscle-invasive status of bladder cancer before surgery is critical due to differences in available treatment options. Therefore, radiologists play an important role in preoperative imaging, according to Qian Cai, MD, co-author of Sun Yat-Sen University.
“It is essential to know whether or not the cancer is muscle invasive due to the severity of the treatments,” Dr. Cai said. “Muscle-invasive bladder cancer should be treated with radical cystectomy, while the treatment of non-muscle-invasive bladder cancer is less aggressive. “The high complication rate and low quality of life after radical cystectomy surgery makes it essential to determine the muscle-invasive status of bladder cancer before surgery.”
More evaluation is needed to continue studying bladder cancers located at the ureteral orifice.
“The VI-RADS score, specifically the 1 to 2 cutoff versus the 3 to 5 cutoff, could be used to accurately predict muscle-invasive bladder cancer. Further evaluation of this scoring system is warranted,” Dr. Wang said.
For more information
Access the Radiology study, “ Multiparametric MRI Evaluation of VI-RADS for Bladder Tumors Located at the Ureteral Orifice .”















