
Highlights
|
Background
The American College of Cardiology/American Heart Association guidelines recommend evaluation and classification of the severity of aortic stenosis (AS) as mild, moderate, or severe , by echocardiogram, and recommend aortic valve replacement (AVR) when AD is serious .
Goals
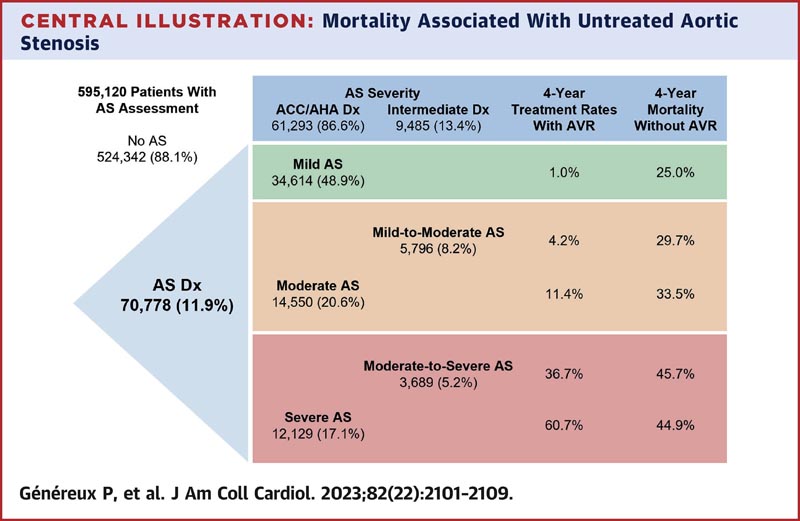
The authors sought to describe mortality rates across the spectrum of untreated aortic stenosis (AS) from a large contemporary real-world database.
Methods
We analyzed a real-world de-identified data set including 1,669,536 echocardiographic reports (1,085,850 patients) from 24 US hospitals (eginte Database, egnite). Patients older than 18 years were classified according to the severity of the AD diagnosis.
Mortality and treatment-untreated rates were examined with Kaplan-Meier (KM) estimates, and results were compared using the log-rank test. Multivariate risk analysis was performed to evaluate associations with all-cause mortality.
Results
Among 595,120 patients with available AD severity assessment, the 4-year Kaplan-Meier (KM)-estimated, unadjusted, untreated, all-cause mortality associated with an AD diagnosis of none, mild, mild to moderate, moderate, moderate to severe or severe was 13.5% (95% CI: 13.3%-13.7%), 25.0% (95% CI: 23.8%-26.1%), 29. 7% (95% CI: 26.8%-32.5%), 33.5% (95% CI: 31.0%-35.8%), 45.7% (95% CI: 37.4 %-52.8%) and 44.9% (95% CI: 39.9%-49.6%), respectively.
The results were similar when adjusted for informational censoring caused by the treatment.
Observed 4-year treatment rates estimated by Kaplan-Meier (KM) were 0.2% (95% CI: 0.2%-0.2%), 1.0% (95% CI: 0.7% -1.3%), 4.2% (95% CI: 2.0%-6.3%), 11.4% (95% CI: 9.5%-13.3%), 36.7 % (95% CI: 31.8%-41.2%) and 60.7% (95% CI: 58.0%-63.3%), respectively. After adjustment, all AD severity grades were associated with increased mortality.
Conclusions Patients with aortic stenosis (AS) have a high risk of mortality at all levels of untreated AS severity . Aortic valve replacement rates remain low for patients with severe AS, suggesting that more research is needed to understand barriers to diagnosis and the appropriate approach and timing for aortic valve replacement. |















