Background
Treatment of gestational diabetes improves maternal and infant health, although diagnostic criteria remain unclear.
Methods
We randomly assigned women at 24 to 32 weeks’ gestation in a 1:1 ratio to evaluate gestational diabetes using lower or higher glycemic criteria for diagnosis.
The criterion for lowest blood glucose was a fasting plasma glucose level of at least 92 mg per deciliter (≥5.1 mmol per liter), a 1-hour level of at least 180 mg per deciliter (≥10.0 mmol per liter), or a 2-hour level of at least 153 mg per deciliter (≥8.5 mmol per liter).
The highest glycemic criterion was a fasting plasma glucose level of at least 99 mg per deciliter (≥5.5 mmol per liter) or a 2-hour level of at least 162 mg per deciliter (≥9.0 mmol per liter). liter).
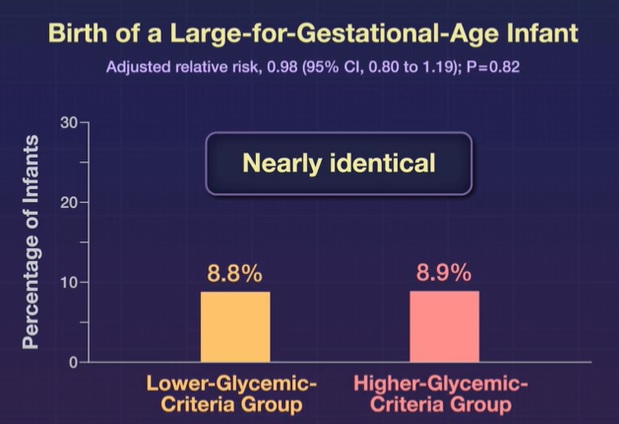
The primary outcome was the birth of a large-for-gestational-age baby (defined as a birth weight above the 90th percentile according to Fenton and World Health Organization standards).
Results
A total of 4061 women were randomized. Gestational diabetes was diagnosed in 310 of 2022 women (15.3%) in the lower glycemic criteria group and in 124 of 2039 women (6.1%) in the higher glycemic criteria group.
Among 2,019 infants born to women in the lowest glycemic index criteria group , 178 (8.8%) were large for gestational age, and among 2,031 infants born to women in the highest glycemic index criteria group , 181 (8.9%) were large for gestational age (adjusted relative risk, 0.98; 95% confidence interval, 0.80 to 1.19; P = 0.82).
Induction of labor, use of health services, use of pharmacological agents, and neonatal hypoglycemia were more common in the lower glycemic criteria group than in the higher glycemic criteria group.
Secondary outcomes were similar in the two test groups, and there were no substantial differences between the groups in adverse events.
Among women in both groups whose glucose test results fell between the lowest and highest glycemic criteria , those who were treated for gestational diabetes (195 women), compared with those who were not (178 women), had benefits in maternal and child health including fewer large for gestational age babies.
Conclusions Using lower glycemic criteria for diagnosing gestational diabetes did not result in a lower risk of a large-for-gestational-age baby than using higher glycemic criteria . |
(Funded by the New Zealand Health Research Council and others; GEMS Australian and New Zealand clinical trials registration number, ACTRN12615000290594. opens in new tab.)















