
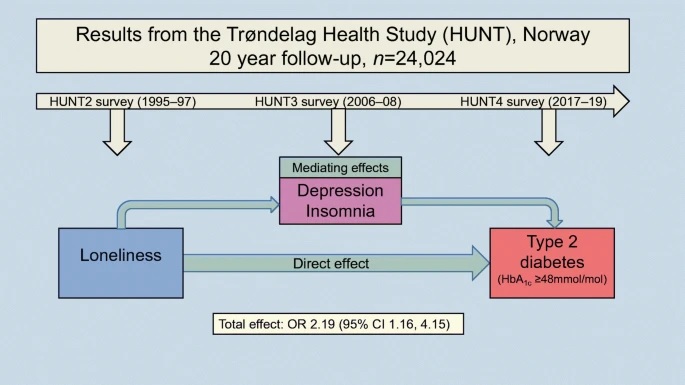
Summary Objectives/hypotheses Type 2 diabetes is a leading cause of death worldwide and its incidence has increased dramatically over the past two decades. Recent research suggests that loneliness is a possible risk factor for type 2 diabetes. This 20-year follow-up study examined whether loneliness is associated with an increased risk of type 2 diabetes. Since both loneliness and type 2 diabetes have been linked to depression and sleep problems, we also investigated whether any association between loneliness and type 2 diabetes is mediated by symptoms of depression and insomnia. Methods We used data from the Trøndelag Health Study (HUNT study), a large, population-based longitudinal health study in central Norway (n=24,024). Self-reports of loneliness (HUNT2 survey, 1995-1997) and data on HbA1c levels (HUNT4 survey, 2017-2019) were analyzed to assess associations between loneliness and incidence of type 2 diabetes. Associations were reported as OR with 95% CI, adjusted for sex, age and education. We further investigated the role of depression and insomnia as possible mediating factors. Results Over the 20-year follow-up period, 4.9% of study participants developed type 2 diabetes. 12.6% of participants reported varying degrees of feeling lonely. People who felt loneliest had twice the risk of developing type 2 diabetes relative to those who did not feel lonely (adjusted OR 2.19 [95% CI: 1.16, 4.15]). The effect of loneliness on type 2 diabetes was weakly mediated by insomnia subtype but not by depressive symptoms. Conclusions/interpretation This study suggests that loneliness may be a factor that increases the risk of type 2 diabetes; however, there is no strong support that the effect of loneliness on type 2 diabetes is mediated by depression or insomnia. We recommend that loneliness be included in clinical consultation and intervention guidelines related to type 2 diabetes. |
Comments
A new study published in Diabetologia (the journal of the European Association for the Study of Diabetes [EASD]) finds that feelings of loneliness are linked to a significantly increased risk of developing type 2 diabetes (T2D).
The research was conducted by Associate Professor Roger E. Henriksen and colleagues at the Western Norway University of Applied Sciences. In addition to examining the association between loneliness and the risk of developing T2D, it looked at whether depression and insomnia play a role.
A growing body of research has pointed to a link between psychological stress and a person’s risk of developing T2D. Loneliness creates a chronic and sometimes long-lasting state of distress that can activate the body’s physiological stress response. While the exact mechanisms are not fully understood, this response is thought to play a central role in the development of T2D through mechanisms such as temporary insulin resistance caused by elevated levels of the stress hormone cortisol.
This process also involves changes in the brain’s regulation of eating behavior, leading to an increased appetite for carbohydrates and subsequent elevated blood sugar levels. Previous studies have found an association between loneliness and unhealthy eating, including increased consumption of sugary drinks and foods high in sugar and fat.
The researchers used data from the HUNT study, a collaboration between the HUNT Research Center (Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology [NTNU]), Trøndelag County Council, the Regional Health Authority of Central Norway and the Norwegian Institute of Public Health. This database contains health information (from self-reported questionnaires, medical examinations and blood samples) of more than 230,000 people and obtained through four population surveys: HUNT1 (1984-1986), HUNT2 (1995-1997 ), HUNT3 (2006-2008). ) and HUNT4 (2017-2019).
Baseline information for 24,024 participants was taken from HUNT2 after excluding people with metabolic disorders, type 1 and type 2 diabetes and those for whom blood test data were not available. T2D status was the primary outcome variable and was based on HbA1c (glycated hemoglobin, a measure of long-term blood sugar control) being greater than 48 mmol/mol when measured in the HUNT4 survey.
Loneliness was measured from the HUNT2 survey data if they had felt lonely during the previous 2 weeks and was measured on a four-point scale ( ’ not’, ’a little’, ’a good amount’, and ’a lot’. ’ ).
Depression symptom severity was assessed using a questionnaire completed during HUNT3 consisting of 7 questions, each scored on a scale of 0 to 3 for a total of 0 to 21 points, with higher scores indicating more severe symptoms.
People with insomnia were identified based on their responses to the questions: ’How often in the past 3 months did you: ’have difficulty falling asleep at night’, ’wake up repeatedly during the night’, and ’have woke up too early and couldn’t go back to sleep’, respectively. These were done as part of HUNT3 and participants could choose one of three responses: “never/rarely,” “sometimes,” and “several times a week . ”
Of 24,024 people, 1,179 (4.9%) developed T2D during the course of the study (1995-2019). These individuals were more likely to be men (59% vs. 44%) and had a higher mean age (48 years vs. 43 years) than those without T2D. They were also more likely to be married (73% vs. 68%) and have the lowest level of education (35% vs. 23%). Feelings of loneliness were reported by 13% of participants.
The study found that higher levels of loneliness at baseline were strongly associated with a higher risk of T2D when measured 20 years later.
After adjusting for age, sex, and educational level, they found that participants who answered "a lot" when asked if they had felt lonely were twice as likely to develop T2D as those who did not feel lonely. Further analysis showed that this relationship was not altered by the presence of depression, sleep onset insomnia, or terminal insomnia, although the team found evidence of a link with sleep maintenance insomnia.
Although their study did not examine the exact mechanisms involved, the researchers note that social support, influence and commitment can have positive effects on health-promoting behaviors. For example, advice and support from a friend can influence a person’s health-related choices and have a positive effect on their diet, physical activity level, and overall feelings of stress. Fewer social ties and a lack of these positive influences can make lonely people more vulnerable to behaviors that could increase the risk of developing T2D.
Researchers advise that loneliness be included in clinical guidelines related to T2D. They say: “It is important for healthcare providers to be open to dialogue about an individual’s concerns during the clinical consultation. tions, including with respect to loneliness and social interaction.”
The authors recommend that more research be conducted into the mechanisms involved in the link between loneliness and type 2 diabetes, as well as the roles played by insomnia and depression. They conclude: "The questions that need to be answered are to what extent loneliness leads to the activation of stress responses, to what extent loneliness affects health-related behavior, and, most importantly, how these two pathways interact in terms of of contributing to a higher risk of T2D.”















