
This randomized trial evaluated the effect of high-intensity interval training (HIIT) on coronary atheromatous plaques in 60 patients with stable coronary artery disease after PCI. Twice-weekly sessions of supervised HIIT at 85% to 95% of maximum heart rate compared to contemporary standards of care for 6 months were associated with a significant reduction in intravascular ultrasound-derived percent atheroma volume and the total atheroma volume normalized for the segment length.
These findings suggest that HIIT is associated with regression of atheroma volume among patients with stable coronary artery disease after PCI, with implications for secondary preventive efforts.
- In patients with established CAD, regression of atheroma volume was observed in those who underwent supervised HIIT for 6 months compared to patients who followed current preventive guidelines.
- In just 6 months, VO2peak improved significantly after HIIT, but not in the control group.
- There was a considerable reduction in body mass index and waist circumference in the HIIT group compared to the control group.
Coronary atheroma volume is associated with the risk of coronary events in coronary artery disease (CAD). Exercise training is a cornerstone in the primary and secondary prevention of CAD, but the effect of exercise on coronary atheromatous plaques is largely unknown.
We evaluated the effect of six months of supervised high-intensity interval training (HIIT) on coronary plaque geometry using intravascular ultrasound in patients with stable CAD after percutaneous coronary intervention (PCI).
Sixty patients were randomized to two weekly sessions of supervised HIIT at 85-95% of maximum heart rate (n = 30) or to follow contemporary preventive guidelines (control group, n = 30).
The endpoints of the study were the change in percent atheroma volume (PAV) and total atheroma volume (TAV) normalized for segment length (TAVnorm) at six-month follow-up.
The change in mean PAV for paired coronary segments from baseline to follow-up showed a significant difference between groups (-1.4, 95% CI -2.7 to -0.1, p = 0.036).
There was a significant reduction in the HIIT group (-1.2, 95% CI -2.1 to -0.2, p = 0.017) while not in the control group (0.2, 95% CI : -0.7 to 1.1, p = 0.616). TAVnorm was reduced (-9 mm3, 95% CI: -14.7 to -3.4, p = 0.002) after HIIT, with a significant difference between groups (-12.0 mm3, 95% CI: - 19.9 to -4.2, p = 0.003).
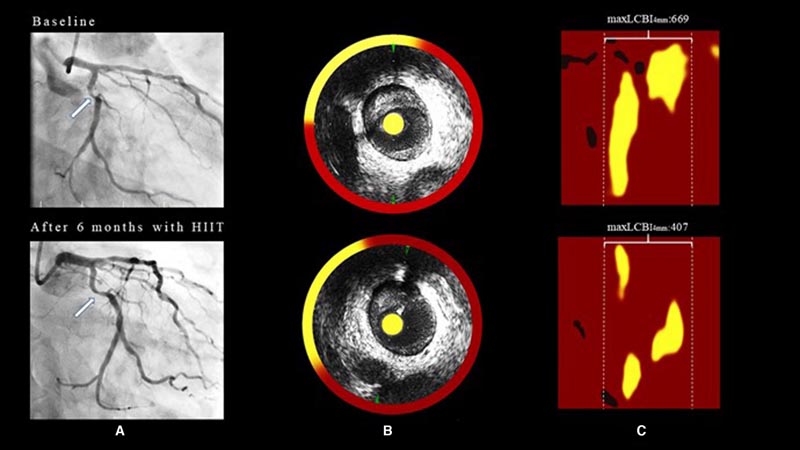
Figure : Case demonstrating vessel imaging findings with coronary angiography and near-infrared spectroscopy combined with intravascular ultrasound (NIRS-IVUS) in a patient in the high-intensity interval training group at baseline (upper panel) and in the follow-up (bottom panel). A, Coronary angiography with arrow showing plaque in the proximal segment of the circumflex artery. B, Cross section of NIRS‐IVUS image where yellow circumferential rings represent lipid accumulation within the plaque. C, NIRS chemogram demonstrating maxLCBI4mm at baseline and follow-up with a reduction in maxLCBI4mm from 669 to 407 during the intervention period. Yellow represents a high probability of lipid and red indicates no lipid. HIIT indicates high intensity interval training; and maxLCBI4mm, maximum core lipid loading index within any 4 mm segment across the entire lesion.
In patients with established coronary artery disease (CAD), regression of atheroma volume was observed in those who underwent six months of supervised HIIT compared to patients who followed contemporary preventive guidelines.
Our study indicates that high-intensity interval training counteracts the progression of atherosclerotic coronary disease and reduces atheroma volume in residual coronary atheromatous plaques after PCI.
Physical exercise after percutaneous coronary intervention in patients with stable coronary artery disease can reduce the lipid content in coronary atheromatous plaques evaluated by near-infrared spectroscopy with a possible positive correlation between the increase in VO2max and the reduction in lipid content. lipids.
A lipid-lowering effect of physical exercise on coronary atheromatous plaques reinforces the scientific evidence to recommend physical exercise in rehabilitation programs.
Physical exercise is highly recommended for the secondary prevention of coronary artery disease (CAD) and multiple beneficial biological effects have been demonstrated with regular physical exercise. Furthermore, several studies have demonstrated strong, positive associations between the level of physical exercise and life expectancy in both healthy subjects and patients with CAD. However, the survival benefit of regular physical exercise has not been demonstrated in randomized clinical trials in CAD.
There is a paucity of data on the effect of physical exercise on atheromatous plaques in coronary arteries. Studies in athletes with coronary computed tomography angiography indicate that strenuous physical exercise is associated with increased calcium in the coronary arteries. Data on the effect of physical exercise on plaque volume, plaque composition, and plaque vulnerability are modest.
Using intravascular radiofrequency ultrasound, we previously demonstrated a reduction in necrotic core following a period of exercise training in patients with CAD. Furthermore, we demonstrated that plaque vulnerability after an exercise intervention could change in different directions within the same patient, indicating factors affecting plaque composition. Near-infrared spectroscopy ( NIRS) can be used to determine the lipid content in atheromatous plaques of coronary arteries.
Previous studies have shown that lipid-rich lesions are more vulnerable and, together with plaque volume, represent a higher risk of future cardiac events, also recently demonstrated in the PROSPECT 2 trial (Providing Regional Observations to Study Predictors of Events). in the Coronary Tree ). With the use of NIRS, pharmacotherapy studies with lipid-lowering drugs have confirmed a favorable reduction in the levels of lipid content in the coronary arteries.
No previous trial has investigated the effect of physical exercise on lipid content in coronary arteries. In this trial, we hypothesized that lipid content in coronary atheroma plaques assessed with near-infrared spectroscopy (NIRS) would be reduced after a period of regular high-intensity interval training (HIIT) compared to usual care. .
To date, only a few studies have used intracoronary imaging when evaluating the effects of exercise. Data derived from this study indicate that HIIT counteracts the progression of atherosclerotic coronary disease and reduces atheroma volume in residual coronary atheromatous plaques after PCI.
These findings are important contributions to understanding the influence of exercise on DKA. The study also confirms the ability of exercise, especially HIIT, to improve cardiovascular health with substantial increases in VO2peak and reductions in body mass index. These results reinforce the scientific basis for recommending physical exercise as an essential component of cardiac rehabilitation programs.















