Sciatic nerve injury from an intramuscular (IM) injection into the buttock is potentially devastating.
In severe cases, the hamstrings and all the muscles below the knee become paralyzed, resulting in a numb, shaking foot. This preventable complication has been known since the 1920s and is highlighted in the nursing research literature.
However, most physicians are involved in prescribing medications that can be administered by intramuscular injection (e.g., vaccines, vitamins, steroid hormones, analgesics, and major tranquilizers), and safe injection practices should be of concern to all practitioners. Of the health.
The objectives of this study were twofold: to establish whether sciatic nerve injury due to intramuscular injection is an ongoing problem and to determine the availability of published guidelines on intramuscular injection techniques within nursing organizations in the UK, USA. and Australasia.
Background/objectives:
An intramuscular (IM) injection into the buttock risks damaging the sciatic nerve. Both doctors and nurses should understand safe injection practices. The objectives of this study were to determine whether sciatic nerve injury due to IM injection is an ongoing problem and to establish the availability of published guidelines on IM injection techniques.
Methods:
Claims for intramuscular injection-related sciatic nerve injuries to the New Zealand Accident Compensation Corporation between July 2005 and September 2008 were reviewed.
Nursing organizations were surveyed to ask about guidelines on IM injection. Sciatic nerve injuries related to intramuscular injection were systematically reviewed in the medical and medicolegal literature (1989-2009).
Results:
There were eight claims for sciatic nerve injection injuries made to the ACC during the 3-year study period; all were in young adults. Only one of the nursing organizations contacted had published guidelines on IM injection technique, and these related specifically to immunization.
Seventeen reports of patients with sciatic nerve injury by intramuscular injection were identified comprising a total of 1506 patients, at least 80% of whom were children .
Nine judicial decisions were identified that ruled in favor of the plaintiff, all from the North American legal system. A wide range of drugs were implicated in the offending intramuscular injections.
Conclusions:
Sciatic nerve injury from an intramuscular injection in the upper outer quadrant of the buttock is a preventable but persistent global problem, affecting patients in both rich and poor health systems. The consequences of this injury are potentially devastating.
There are safer alternative sites for IM injection. These should be promoted more widely by medical and nursing organizations.
Message for practice
Avoid the upper outer quadrant of the buttock for intramuscular injection due to the risk of sciatic nerve injury.
For vaccinations, use recommended alternative sites. For medications that must be administered by intramuscular injection, the ventrogluteal area is safer.
Discussion
Iatrogenic injury to the sciatic nerve as a result of incorrect intramuscular injection into the buttocks is a persistent global problem affecting patients from economically rich and poor countries alike, although with a different spectrum of affected individuals. In economically poorer countries, children make up the largest number of reported cases.
In a national study conducted in Pakistan between 2001 and 2003, the estimated annual incidence of traumatic injection neuropathy (more than 90% of which involved the sciatic nerve) was 7.1 per million children under 3 years of age. In countries such as Pakistan, India and Nigeria, the administration of intramuscular injections by untrained or unqualified personnel appears to be a major cause.
The problem is compounded by mistaken beliefs that IM injections work faster or reflect better quality care.
The effects of injection-related sciatic nerve injury are variable, ranging from transient sensory disturbances to permanent paralysis and numbness. Affected children may not be able to walk or crawl; a significant proportion has foot drop. The common fibular component of the sciatic nerve is most commonly affected due to its posterolateral position and less supporting connective tissue. Anatomical variations in the course and division of the sciatic nerve may be a factor in some cases.
Affected patients typically experience immediate pain that radiates down the extremity, with weakness and numbness that evolves more gradually, exacerbated by secondary scarring. The degree of recovery depends on the severity of the initial injury. Many patients fail to make a full recovery, even with the benefit of microsurgical repair.
| Common sites for IM injection are the anterolateral thigh, deltoid, and gluteal regions . The latter can be subdivided into the dorsogluteal (commonly known as the upper outer quadrant of the buttock) and the ventrogluteal (between the iliac crest, the greater trochanter of the femur and the anterior superior iliac spine). |
Immunization guidelines in the UK, US and Australia recommend that the buttocks not be used for intramuscular injection due to the risk of sciatic nerve injury; instead, the anterolateral thigh in infants or the deltoid region in older children should be used.
In general, a warning is added that the upper outer quadrant of the buttock can be used for large volume IM injections. However, immunizations aside, the potentially dangerous dorsogluteal site is still widely used for IM injection of medications and continues to be recommended in nursing texts and clinical practice.
The buttocks are an attractive site for intramuscular injection due to their obvious volume (muscle), but the term "upper outer quadrant" lacks precision. The buttock is defined as ’one of the two protuberances of the tailbone’, while the gluteal region extends between the iliac crest at the top and the gluteal crease at the bottom from the midline posteriorly to a line that joins the greater trochanter of the femur. and anterior superior iliac spine laterally.
Using the dorsogluteal region not only risks damage to the sciatic nerve, but it is also not a good site for intramuscular injection.
In a study of 100 consecutive adults, the depth of adipose tissue in this region exceeded the 35 mm limit of a 21 g needle (green) in 43%. In another study of 50 hospitalized patients who received an IM injection into the "upper outer quadrant" of the buttock with a 30-mm-long needle, the injections were IM in only 32% of patients (8% in women); the majority were subcutaneous.
No IM injection site is without risk, including the anterolateral thigh and deltoid regions. In the gluteal region, the ventrogluteal area (Figure 1) is safer, with only one significant complication reported. This site has less subcutaneous fat, offers the combined thickness of the gluteus medius and minimus muscles, has relatively fewer nerves and blood vessels, and can be accessed with the patient on their side or supine.
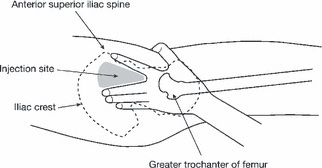
The gluteal triangle for IM injection (ventrogluteal region). The palm of the opposite hand is placed on the greater trochanter and the index finger on the anterior superior iliac spine. A triangle is formed with the middle finger pointing towards the iliac crest. The injection site is the center of the triangle, with the needle inserted at 90° to the skin surface.
Despite this, nurses have been reluctant to use this site; A recent survey in New Zealand showed that only 9% of nurses had used this site. This may be due in part to a lack of confidence in area identification. Perhaps the cumbersome term "ventrogluteal" should be replaced with an alternative, such as the "gluteal triangle" , to avoid confusion with the dorsogluteal region and the gluteus.















